Journal Name: Journal of Biomedical Research and Reviews
Article Type: Case Report
Received date: 10-February-2021
Accepted date: 12-March-2021
Published date: 19-March-2021
Citation:Deng S, Yin Q, Zhu H, Lu J (2021) A primary Pulmonary Glomus Tumor: A Case Report and Literature Review. J Biomed Res Rev Vol: 4, Issu: 1 (18-21).
Copyright: © 2021 Lu J et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Primary pulmonary glomus tumor is rare and only 36 cases have been reported in the English literature until 2016. The clinical manifestations are related symptoms occupying lesions in the lung. The diagnosis of the tumor depends on histopathology and immunohistochemistry. Surgical resection is considered as the most effective treatment for this condition.
We report a case of old patient whose final diagnosis was primary pulmonary glomus tumor. She initially was found a nodule in the right lung, which was enlarged during follow-up and finally confirmed after surgery. Postoperative pathology was considered as a primary pulmonary glomus tumor. There has been no evidence of tumor recurrence or metastasis so far.
Keywords
Glomus tumor, Lung tumors, Surgical resection.
Abstract
Primary pulmonary glomus tumor is rare and only 36 cases have been reported in the English literature until 2016. The clinical manifestations are related symptoms occupying lesions in the lung. The diagnosis of the tumor depends on histopathology and immunohistochemistry. Surgical resection is considered as the most effective treatment for this condition.
We report a case of old patient whose final diagnosis was primary pulmonary glomus tumor. She initially was found a nodule in the right lung, which was enlarged during follow-up and finally confirmed after surgery. Postoperative pathology was considered as a primary pulmonary glomus tumor. There has been no evidence of tumor recurrence or metastasis so far.
Keywords
Glomus tumor, Lung tumors, Surgical resection.
Introduction
Pulmonary glomus tumors are a rare benign tumor of the lung [1]. Histologically, it is composed of small blood vessels and surrounding tumor cells. This disease is relatively rare, and there are few reports in China. The diagnostic and therapeutic strategies for this have not been well established [2]. Here we reported a case of primary pulmonary glomus tumor in right upper lobe of lung, including its pathological features, and reviews the related literature to improve the understanding of the tumor.
Case Presentation
A 63-year-old female presented to our hospital with a lung nodule at the right upper lobe (RUL), which were detected at a different institution during an examination for intermittent cough. This mass was first discovered in 2014, when the patient was admitted to the hospital for physical examination. The patient was advised to be submitted in surgical resection of the mass, due to its location in the superior lobe of right lung. At that time, the size of the nodules was 12mm*13mm. She refused the surgery and since then the mass was under surveillance with computer tomography of the thorax every year.
The patient’s past medical history was significant for diabetes mellitus, with a history of cholecystectomy. Physical examination and routine laboratory tests revealed no significant findings. A chest computed tomography (CT) scan revealed a 15.4mm*13mm sized mass in the apical segment of the right upper lobe (Figure 1). Bronchoscopy showed no endobronchial involvement. As the pulmonary function test indicated no contraindication, we recommended surgery because of the possibility of malignancy in the nodule. We performed an upper lobectomy with mediastinal lymph node dissection by the thorax surgery. With pathologic examination, it was demonstrated to be a primary pulmonary glomus tumor of uncertain malignant potential. The patient was discharged from the hospital without any complications on postoperative day eight.
Figure 1
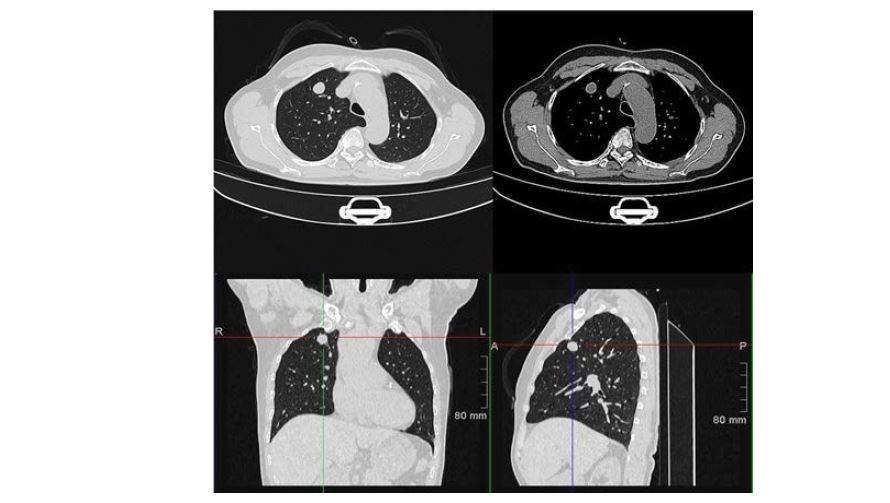
Figure 1: CT scans showed a well-marginated mass in the apical segment of the RUL.
Grossly, wedge resection of right lung, a mass was found in the pulmonary parenchyma, 3mm away from the pulmonary membrane. Tumor size was 15mm in diameter, appear as well-defined, yellow to red, firm, solid masse. Hematoxylin and eosin (H&E) staining demonstrated that the tumor cells surrounded the blood vessels and grew in a circular, oval and spindle shape. The cytoplasm was rich in eosinophils and pale, several obvious cavernous blood vessels could be observed. In a small area, some atypical features such as pleomorphism could be observed, but the mitotic figures less than 5/50 high power field (HPF). Therefore, the diagnosis of glomus tumor of uncertain malignant potential was confirmed (Figure 2). Immunohistochemically, vimentin for mesenchymal tissues origin (+), SMA and H-Caldesmon for tumors of smooth muscle origin(+), CK and EMA for tumors of epithelial origin(-), CD34 for vascular tumors(-), CD31 for endothelial cells and tumor angiogenesis(-), S-100 and Nestin for nervous tissue origin(-), CgA, CD56 and Syn for tumors of neuroendocrine cells origin(-), Melan-A and HMB- 45 for melanin tissue origin(-), Ki-67 for cell proliferation in tumors(+,10%).
Based on these pathological findings, the final diagnosis was a glomus tumor in the RUL. The patient has remained healthy and is currently in follow-up at an outpatient setting.
Discussion
Glomus tumor is a relatively rare soft tissue tumor, which is characterized by vascular hyperplasia with perivascular hyperplasia and glomerular cells [2]. Most of them occur in the dermis and subcutaneous tissue of the limbs [3]. It has been reported that glomus tumors occur in areas where has never been seen, including bone and the chest wall, eyelid, colon, rectum, cervix, and respiratory tract [4]. Glomus tumors can divide into multiple and isolated type Clinically. Multiple tumors are more common in children and are considered to be a hereditary disease. The mass is often unencapsulated and the vascular lumen is large, which is similar to cavernous hemangioma. Solitary masses often have a capsule and the vascular lumen is small. Glomus tumors of the respiratory tract are located in the large airway, especially the trachea, and are rarely found in the parenchyma of the lungs. Primary pulmonary glomus tumor is very rare. Here, we report a case of primary pulmonary glomus tumor that loomed into apical segment of the right upper lobe.
The exact incidence of primary glomus tumor is not clear. These tumors are usually benign, but in rare cases they may show uncertain or malignant behavior [1,5]. Malignant tumors are more common in the lung than in extrapulmonary. These tumors always demonstrate some malignant histological features, such as cytologic atypia, necrosis, increased mitotic rate and characteristically cystic degeneration [6]. Occasional fatal distant metastases have been reported [2,7].
Criteria for the diagnosis of malignancy glomus tumors was proposed by Folpe in 2001 [8]. Folpe et al classified this tumor into four main types (malignant glomus tumor, symplastic glomus tumor, glomus tumor of uncertain malignant potential, and glomangiomatosis) and elaborated pathologic criteria for malignancy in these tumors [8]. In our case, the tumor was located in the parenchymal organs with a deeper location, some with moderate to high nuclear grade, but its diameter was less than 20mm, and mitotic figures was less than 5/50HPF. Based on the results of H&E staining and immunohistochemistry, the pathological diagnosis was finally confirmed.
Primary pulmonary glomus tumors may present with different clinical manifestations due to the different sites involved. Bronchial glomus tumor showed a prominent polypoid mass, whereas pulmonary glomus tumor showed nodular lesions [9]. The former can often cause airway irritation and obstruction, whereas the latter is usually asymptomatic and found incidentally [2]. Takashi showed a case is a central type of glomus tumor of the lung presenting as pneumonia due to airway obstruction [10]. In our case, this tumor focuses on the lung parenchyma and has no bearing on the airway, wherein our patient emanates from intermittent mild cough without central airway obstruction.
Figure 2
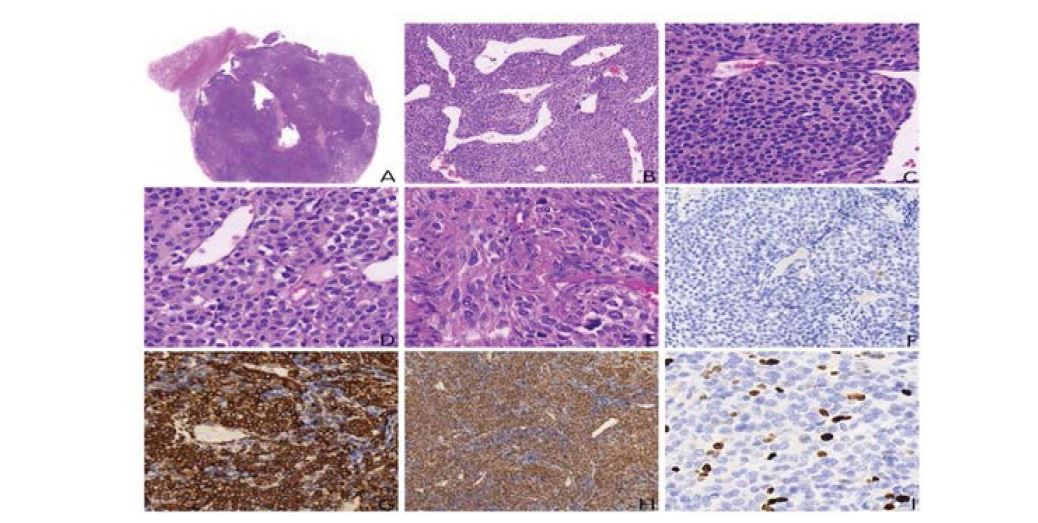
Figure 2: Histopathologic findings : H&E staining. (A) low-power magnification demonstrates fibrous capsule (10×). (B) tumor cells of lung, adjacent to vessels (200×). (C) relatively uniform polygonal cells with oval to round nuclei, eosinophilic cytoplasm, and distinct cell borders (400×). (D) some tumor cells with pale cytoplasm (400×). (E) Marked nuclei and prominent nucleoli in present with mitotic activity (400×). (F) tumor cells were negative for Melan A (400×). (G) the round to spindle cells react strongly with H-Caldesmon (400×). (H) tumor cells of lung showed strong immunoreactivity for smooth muscle actin (200×). (I) the proliferation indexes of tumor cells labelled by Ki-67 protein was 10% (400×).
Primary pulmonary glomus tumors often present as a round, well-defined mass on X-ray or CT scan [11]. They can appear either as single or multiple lesions [3,4,12,13]. Single glomus tumor is more common in adults than in other age groups. On CT scan, there are peripheral numismatic lesions, solitary round nodules and solid or irregular masses accompanied by peripheral small nodules. The boundary is clear or rough, which may be lobulated, with uniform or uneven density, without calcification or cavity. On contrastenhanced CT scan, there are remarkable enhancement on the edge and low-density area in the center [14]. Magnetic Resonance Imaging (MRI) showed equal T1 and high T2 signals in most tumors, and high T1 and T2 signals in the center. Enhanced MRI staked out significant early peripheral enhancement, gradually extending to the central part of the tumor, in which the prized enhancement was out of sight [15]. Positron emission tomography-computed tomography (PET-CT) is round or irregular soft tissue mass showed low to medium intensity nuclide aggregation or no aggregation [3]. In this case, CT findings are similar. The imaging differential diagnosis consists of a wide variety of neoplasms, most notably: carcinoid tumor, hemangiopericytoma, paraganglioma, smooth muscle neoplasms and metastatic tumors.
The proper treatment for primary pulmonary glomus tumors is surgical resection [10]. Most patients received lobectomy or wedge-shaped lung. In addition, mediastinal lymphadenectomy was performed in some patients. The patients were treated with chemotherapy. Malignant glomus tumor is considered as low grade. Malignant local sarcoma, rarely metastasis. Metastasis, as culprit of death of malignant glomus tumor, of which transfer rate was around 31.2%-38% [8]. Therefore, once the diagnosis of malignant glomus tumor identified, the patients should be followed up closely [2].
Conclusion
We reported a case of primary pulmonary glomus tumor in right upper lobe of lung, including its pathological features, and review the related literature to improve the understanding of the tumor. The accurate diagnosis was a challenge both for clinicians and for pathologists.
Ethical Statement
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. Institutional approval was not required for this manuscript.
Disclosure
The authors declare no competing interests.
Funding
This work was supported by Clinical Plateau Discipline Project in Shanghai Pudong New Area (grant number: PWYgy2018-06).

View pdf
Download pdf
Wan PZ, Han Q, Wang EH, Lin XY (2015) Glomus tumor of uncertain malignant potential of the lung: a case report and review of literature. Int J Clin Exp Pathol 8: 15402-15406. [ Ref ]
Oide T, Yasufuku K, Shibuya K, Yoshino I, Nakatani Y, et al. (2016) Primary pulmonary glomus tumor of uncertain malignant potential: A case report with literature review focusing on current concepts of malignancy grade estimation. Respir Med Case Rep 19: 143-149. [ Ref ]
De Coker J, Messaoudi N, Waelput W, Van Schil PEY (2008) Intrapulmonary glomus tumor in a young woman. Interact Cardiovasc Thorac Surg 7: 1191-1193. [ Ref ]
Concatto NH, Irion KL, Marchiori E, Gosney JR, Asante-Siaw J, et al. (2014) An unusual cause of multiple pulmonary nodules: glomus tumors of the lung. Lung 192: 629-630. [ Ref ]
Pardo SS, Duque J, Fajardo JE (2016) Glomus tumor in teen and repetition pneumonia: Case report. Respir Med Case Rep 19: 169-172. [ Ref ]
Choi YJ, Yang KH, Gang SJ, Kim BK, Kim SM (1991) Malignant glomus tumor originating in the superior mediastinum-an immunohistochemical and ultrastructural study. J Korean Med Sci 6: 157-163. [ Ref ]
Cunningham JD, Plodkowski AJ, Giri DD, Hwang S (2016) Case report of malignant pulmonary parenchymal glomus tumor: imaging features and review of the literature. Clin Imaging 40: 144-147. [ Ref ]
Folpe AL, Fanburg-Smith JC, Miettinen M, Weiss SW (2001) Atypical and malignant glomus tumors: analysis of 52 cases, with a proposal for the reclassification of glomus tumors. Am J Surg Pathol 25: 1-12. [ Ref ]
- Hartert Marc, Wolf Michael, Marko Christian, Huertgen Martin (2019) Glomus tumor of the trachea - Synopsis of histology & methodology of treatment. Respir Med Case Rep 28: 100905.
Takahashi N, Oizumi H, Yanagawa N, Sadahiro M (2006) A bronchial glomus tumor surgically treated with segmental resection. Interact Cardiovasc Thorac Surg 5: 258-260. [ Ref ]
Altorjay A, Arato G, Adame M, Szanto I, Garcia J, et al.(2003) Synchronous multiple glomus tumors of the esophagus and lung. Hepatogastroenterology 50: 687-690. [ Ref ]
Ariizumi Y, Koizumi H, Hoshikawa M, Shinmyo T, Ando K, et al.(2012) A primary pulmonary glomus tumor: a case report and review of the literature. Case Rep Pathol 2012: 782304. [ Ref ]
Kleontas A, Barbetakis N, Asteriou C, Nikolaidou A, Baliaka A, et al. (2010) Primary glomangiosarcoma of the lung: A case report. J Cardiothorac Surg 5: 76. [ Ref ]
Huang Y, Chen K, Sun K, Cui J, Chen Y, et al. (2013) A primary pulmonary glomus tumor complicated with hyperpyrexia and anemia. Ann Thorac Surg 95: e29-31. [ Ref ]
Ueno M, Nakashima O, Mishima M, Yamada M, Kikuno M, et al. (2004) Pulmonary glomus tumor: CT and MRI findings. J Thorac Imaging 19:131-134. [ Ref ]
