Journal Name: Journal of Pediatrics and Infants
Article Type:Research
Received date:30 May, 2022
Accepted date:16 June, 2022
Published date:23 June, 2022
Citation: Weldemariam KT, Gezae KE, Abebe HT, Tsegay TT (2022) Individual and Community Level Factors of Low Birth Weight in Ethiopia: Evidence from Ethiopian Demographic Health Survey 2016: Multilevel Modeling. J Pediat Infants Vol: 5, Issu: 1 (09-19).
Copyright: 2022 Weldemariam KT et al. This is an openaccess article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Low birth weight is one of the critical issues in Ethiopia that causes many babies’ short- term and long-term health consequences. In Ethiopia, low birth weight is increasing; however, limited evidences of multilevel factors associated with low birth weight in the study setting, Ethiopia.
Objective: The objective of this study was to assess individual and area level factors of Low Birth Weight in Ethiopia: from Ethiopia Demographic and Health Survey 2016.
Method:The data were extracted from the 2016 Ethiopia Demographic and Health Survey. For analysis a sample of 2110 birth weights within five years preceding the survey were included. The analysis was carried out using STATA software version 14. A two level mixed effects logistic regression analysis was used to estimate both the fixed effects of the individual and contextual factors and the random effects of the between cluster difference. Adjusted Odds Ratio with 95% Confidence Interval to express measures of association and Intra Class Correlation to express measures of variation were used.
Results: A total of 2110 children nested within 445 clusters were included in the analysis. Among them, 13% were with low birth weight. The ICC implied 11.7% of the variance in low birth weight was attributable to Area level unobservable factors. At individual level; multiple birth (AOR=2.74; 95%CI: 1.450-5.184), preterm birth (AOR=4.83; 95%CI: 2.644-8.830), anemic mothers (AOR=1.49; 95% CI: 1.069-2.092), six and above birth order (AOR=0.42; 95%CI: 0.242-0.752), mothers with primary educational level (AOR=0.61; 95%CI: 0.418-0.896) and secondary/higher educational level (AOR=0.39; 95%CI: 0.252-0.612) as well as region from Area level were significantly associated with low birth weight.
Conclusion: The results of this study showed that multiple births, anemic mothers, birth order, not-educated mothers and preterm gestational age at birth were significant factors of low birth weight.
Hence, switching off/on the significant factors accordingly could reduce the risk of having low birth weight child.
Keywords: Low birth weight, Anemic mothers, Gestational age.
Abbreviations: AIC: Akaike’s Information criterion; APH: Ante-partum hemorrhage; CSA: Central Statistical Agency; DHS: Demographic health survey; EAs: Enumeration Areas; EDHS: Ethiopian demographic health survey;
ICC: Intra class Correlation; IUGR: Intra-Uterine growth retardation; LBW: Low Birth Weight; MUAC: Mid-Upper Arm Circumference; NBW: Normal Birth Weight; NMR: Neonatal Mortality Rate; AOR: Adjusted Odds Ratio; SNNP Southern Nation, Nationalities and People; VPC: Variance partition coefficient; WHO: World health organization.
Abstract
Background: Low birth weight is one of the critical issues in Ethiopia that causes many babies’ short- term and long-term health consequences. In Ethiopia, low birth weight is increasing; however, limited evidences of multilevel factors associated with low birth weight in the study setting, Ethiopia.
Objective: The objective of this study was to assess individual and area level factors of Low Birth Weight in Ethiopia: from Ethiopia Demographic and Health Survey 2016.
Method:The data were extracted from the 2016 Ethiopia Demographic and Health Survey. For analysis a sample of 2110 birth weights within five years preceding the survey were included. The analysis was carried out using STATA software version 14. A two level mixed effects logistic regression analysis was used to estimate both the fixed effects of the individual and contextual factors and the random effects of the between cluster difference. Adjusted Odds Ratio with 95% Confidence Interval to express measures of association and Intra Class Correlation to express measures of variation were used.
Results: A total of 2110 children nested within 445 clusters were included in the analysis. Among them, 13% were with low birth weight. The ICC implied 11.7% of the variance in low birth weight was attributable to Area level unobservable factors. At individual level; multiple birth (AOR=2.74; 95%CI: 1.450-5.184), preterm birth (AOR=4.83; 95%CI: 2.644-8.830), anemic mothers (AOR=1.49; 95% CI: 1.069-2.092), six and above birth order (AOR=0.42; 95%CI: 0.242-0.752), mothers with primary educational level (AOR=0.61; 95%CI: 0.418-0.896) and secondary/higher educational level (AOR=0.39; 95%CI: 0.252-0.612) as well as region from Area level were significantly associated with low birth weight.
Conclusion: The results of this study showed that multiple births, anemic mothers, birth order, not-educated mothers and preterm gestational age at birth were significant factors of low birth weight.
Hence, switching off/on the significant factors accordingly could reduce the risk of having low birth weight child.
Keywords: Low birth weight, Anemic mothers, Gestational age.
Abbreviations: AIC: Akaike’s Information criterion; APH: Ante-partum hemorrhage; CSA: Central Statistical Agency; DHS: Demographic health survey; EAs: Enumeration Areas; EDHS: Ethiopian demographic health survey;
ICC: Intra class Correlation; IUGR: Intra-Uterine growth retardation; LBW: Low Birth Weight; MUAC: Mid-Upper Arm Circumference; NBW: Normal Birth Weight; NMR: Neonatal Mortality Rate; AOR: Adjusted Odds Ratio; SNNP Southern Nation, Nationalities and People; VPC: Variance partition coefficient; WHO: World health organization.
Introduction
Background
Low birth weight (LBW), which is defined by the world health organization (WHO) as birth weight less than 2500 grams, is associated with a higher risk of neonatal and infant mortality and morbidity, and a greater risk for adverse health outcomes, cognitive development and school performance problems than those born with normal weight. The subcategories of low birth weight are: very low birth weight (VLBW) which is <1500gram, extremely low birth weight (ELBW) which is <1000gram [1-3].
Low birth weight caused due to either preterm (before 37 weeks of gestational age) or intra-uterine growth retardation (IUGR) and poor health care during pregnancy. The IUGR is often as a result of maternal nutrition either before conception or during pregnancy as well as fetal problem [4].
Low birth weight has public health importance including increased neonatal mortality and morbidity, physical and psychomotor development delay. Besides infant LBW are more likely to develop significant disabilities and there are long term health implication of future chronic disease [4]. LBW due to restricted fetal growth affect the person throughout life and is associated with poor growth in childhood and a higher incidence of adult disease, such as type 2 diabetes, hypertension and cardiovascular disease. An additional risk for girls is having smaller babies when they become mothers [5].
Based on Literatures, the factors associated with premature delivery and low birth weight include: socio economic status, maternal education and occupational, residence, maternal anthropometric status such as: maternal stature, Mid Upper Arm Circumference (MUAC) and multiple pregnancies [6,7].
Triggering LBW, previous history of preterm/LBW/ IUGR, maternal age, birth interval, inadequate weight gain in pregnancy, infectious and improper nutrition are other predictors of LBW. From the maternal factors, stress, smoking, and use of alcohol, pollution, violence and genetic factor are some of the determinant factors of LBW [8].
In 2012, the world health assembly resolution endorsed a comprehensive implementation plan on maternal, infant and young child nutrition, which specified six global nutrition targets for 2025. The third target of this policy briefly covers 30 percent reduction of LBW. The goal is to achieve a 30% reduction of the number of infant born with a weight lower than 2500 gram by the year 2025. This would translate in to 3.9 percent relative reduction per year between 2012 and 2025 [9].
Statement of the Problem
About 20 million infants world-wide accounting for 15.5 percent of all births are born LBW, 95.6 percent of them in developing countries. In developing countries 16.5 percent of infants are born LBW, 13 percent in sub Saharan Africa. LBW is a major public health problem in under-resourced settings [10]. There are 15 million preterm birth (PTB) annually, and more than 1 million of infants born preterm die due to early complications. The rate of PTB is increasing, particularly in sub-Saharan Africa and South Asia where over 60 percent of global PTBs occur [11].
Babies born low birth weight are 37 percent more likely to die during infancy compared to those of normal weight if other factors are held constant. Therefore LBW is strongly negatively associated with infant survival [12]. In a study conducted in East Africa, preterm babies and babies with LBW were found to account for 52 percent of newborn deaths in East Africa [13].
Being born with LBW is generally recognized as a disadvantage for the infant, family and country. Preterm birth is a direct cause of 28 percent of the 4 million neonatal deaths that occur globally every year. Direct or indirect, LBW may contribute to 60 percent to 80 percent of all neonatal death. LBW infant are at higher risk of early growth retardation, infection, developmental delay and death during infancy and childhood [14]. Studies have shown that infants weighing less than 2500 gram were approximately 20 times more likely to die than heavier babies [5].
Based on the united nation report in Ethiopia the prevalence pattern of LBW in 2000 GC was 15 percent but in 2005 GC report was 20.5 percent [15]. The pattern of LBW in Ethiopia was increased from 11 percent to 13 percent in 2011 and 2016 respectively. Based on a different researches done in Ethiopia was reported the prevalence of LBW in Addis Ababa 11 percent, and in Jima 22.5 percent and Gondar 17.4 percent and the prevalence of LBW in Tigray was 9.9 percent [3,15,16].
In Ethiopia, using a single level analysis, there are a lot of studies done on LBW, however; the multilevel factors associated with LBW, are not well addressed. For data with a hierarchical nature, using single level logistic regression can bias the parameter estimation. Multilevel models allow one to account for the clustering of subjects within clusters of higher-level units when estimating the effect of subject and cluster characteristics on subject outcomes and gives us appropriate parameter estimation for nested data.
Limited evidences are available regarding predictors of LBW in Ethiopia at nationally representative sample.
So this study has taken a step further from the routine EDHS report by further analysis of DHS data using advanced analysis model to assess multilevel factors of LBW using a multilevel logistic regression model and provides context specific information to program planners and policy makers.
Objectives
General Objective
To assess the individual and Area level factors of low birth weight in Ethiopia evidence from EDHS 2016.
Specific Objectives
To identify the individual level factors associated with low birth weight in Ethiopia EDHS 2016. To identify the Area level factors associated with low birth weight in Ethiopia EDHS 2016.
Methods and Materials
Study setting
The study was conduct in Ethiopia in 2020 from EDHS 2016. According to Ethiopia Demographics Profile 2020, Ethiopia is the second-most populous nation on the African continent with 105,350,020 estimated populations and with 79.6% of its population living in rural areas. Administratively, Ethiopia is divided into nine geographical regions and two administrative cities [3]. The current health policy of Ethiopia gives much more emphasis on prevention and the health promotion components of health care that should be able to resolve most of the health problems of the population [17].
Data source
The child dataset used for this analysis was the 2016 EDHS. It is the latest and the nationally large scale dataset of demographic and health survey that was conducted by the Central Statistical Agency (CSA) from January 18, 2016 to June 27, 2016 with nationally representative sample from 9 regions and two administrative cities. The total study participant to this study was 2110 infants whose weights were recalled. Details of sampling design and selection of sample are available in the Ethiopia Demographic and Health Survey 2016 EDHS reports [3].
Study design
A cross sectional study design was used to identify multilevel factors associated with LBW from the 2016 EDHS data collected by the CSA.
Population
Source population: All live births in the five years born to women’s of reproductive age of 15-49 years who were residents of the nine regions and two administrative cities of Ethiopia during the survey.
Study population: All live births in the five years born to women’s of reproductive age of 15-49 years, who were residents of the selected households in the selected enumeration areas during the survey.
Sample population: All live births in the five years born to women’s of reproductive age of 15-49 years, who were residents of the selected HHs in the selected enumeration areas during the survey, Study population who fulfilled the inclusion criteria.
Eligibility criteria
Inclusion and exclusion criteria: All Birth Weighted infants in EDHS 2016 sampled areas were included in the study. All mothers who had not weighted their children and do not know their child’s weight were excluded.
Operational and standard definition: Normal birth weight- is a weight class greater than or equal to 2500 gram.
Aggregated community level variables: the aggregated community level predictor variables were constructed by aggregating individual level values at cluster level, and binary categorization of the aggregated variables were done based on the distribution of the proportion values calculated for each cluster(community ). Mean for normally distributed or median for not normally distributed community level aggregated predictor variables were used as cut off point for categorization. Histogram was used to check the distribution whether it is normal or not
Interchangeable words: Enumeration areas, Enumeration communities, and clusters are used interchangeably in this document to refer the sampling unit of the higher level unit.
Individual level factors: A variable operating at the lowest level or individual level which included children’s, parents and household characteristics.
Sample size and sampling procedures
EDHS 2016 used a multistage stratified cluster sampling method. The sampling frame used was adopted from the Ethiopia Population and Housing Census of 2007 that had complete list of 84,915 enumeration areas. 2016 EDHS sample was selected in two stages. Each region was stratified into urban and rural areas, yielding 21 sampling strata. Samples of enumeration areas were selected independently in each stratum in two stages. . In the first stage 645 (202 urban communities and 443 rural communities) enumeration areas (clusters) were selected. At second stage 28 households per cluster were selected. All women aged 15-49 years were eligible to be interviewed. Of all the child dataset related to birth weight, 2110 infants were eligible to this study.
Data quality control
Data related to the outcome variable of low birth weight was selected and extracted from the child dataset of EDHS 2016. Further data cleaning, labeling, coding and recoding were done. Categorization was done for continuous and categorical variables using information from different literatures if necessary for comparison with the previous literatures.
Study variables
Dependent variable: The outcome variable is low birth weight. The dependent variable for the ith birth weight was represented by a random variable with two possible values coded 1 and 0. So, the response variable of the ith birth weight was measured as a dichotomous variable. (Yi=1 if low birth weight was occurred, otherwise Yi=0)
Independent variables: This study had individual and community level independent variables.
Individual level variable: Individual level factors considered in this study includes: Age of mother, maternal age at first birth, gestational age at birth, birth order, type of birth, sex of the child, sex of household head, marital status, mother’s educational level, husband/partner educational level, maternal occupation, husband/partner occupation, cigarette smoking, household wealth index, religion, household size, media exposure, body mass index.
Community level variables: In addition to region, place of residence, community media exposure, community educational status and community poverty status were the independent variables considered at community level. The aggregated community level predictor variables were constructed by aggregating individual level values at cluster level and binary categorization of the aggregated variables were done based on the distribution of the proportion values calculated for each cluster (community ) (see operational definition section).
Statistical methods of analysis
Multilevel Modeling: Nature of nested data makes the uses of traditional regression methods inappropriate because of the assumption of independence among individual within the some group, assumption of equal variance across groups which an inherent in traditional regression methods are violated. Therefore, multilevel model is a type of regression analysis for multilevel data where the dependent variable is more appropriate for hierarchically structured data, such as the DHS to estimate the robust standard error. So in this study multilevel binary logistic regression analysis was employed in order to account for the hierarchical nature of the DHS data and the binary response of the outcome variable.
Data analysis: The data was taken from EDHS 2016 and entered into STATA 14 to be analyzed using multilevel logistic regression. A two level logistic regression was assessed for the explanatory effects of the independent variables on LBW by considering the hierarchical nature of data. The first level represents the individual birth weight and the second level the Community where the individual are nested in the Community level covariates are the geographical demarcation of each Enumeration community . Description and analysis of data were addressed by including the following section: descriptive statistics and cross tabulation, multilevel regression analysis and diagnostics. EDHS sample was not self-weighted because of non-proportional allocation of different regions and urban rural residences of the country that often be over sampled in one region and under sampled in other region. Therefore; EDHS sampling weights was used to make the sample representative of the entire population.
Descriptive analysis: Frequency and percentage were used to report categorical variables; mean for continuous normal variables, and median followed by Inter quartile Range, for continuous explanatory variables that violate assumption of normality, were also used. In addition cross tabulation was done to show the proportion of different categories of each characteristic with respect to the outcome variable (Low birth weight)
Multilevel Analysis
Bivariate multilevel logistic regression analysis: Bivariate MLRA was employed to explore association between dependent variable and a wide range of independent variables. Variables with p-value of ≤ 0.25 were considered as potential candidates of multivariable logistic regression analysis [18].
Multivariable Multilevel Logistic Regression Analysis
Multilevel logistic regression model was fitted to examine the individual and community level factors that are associated with low birth weight at p-value of ≤ 0.25 during the bivariate multilevel logistic regression analysis. Variables with p-value of less than 0.05 were considered as significant predictors. The result was presented with odds ratio (AOR) and 95% confidence interval (CI).
Model specification
In this multilevel analysis it has set up of two level models. The level one individual variables and second level is the Community level. This study has already focused on random intercept model in addition to the individual and community level fixed effects. The analytical strategy in the case of multilevel analysis consists of four models.
The first model which is usually called the “empty” or “null model” is fitted without explanatory variables. In other words, it contained no covariates, but decomposes the total variance in to individual and community components. The empty model is used to determine whether the overall difference on LBW between communities was significant.
Y=ln[Pij/1-Pij]=β0j + u0j…………………………(1)
In the above equation, Pij is probability of LBW, β0j is the overall regression intercept when all predictors were adjusted to zero and u0j is the residuals at the community level.
The second model referred to the “individual model” included only individual-level characteristics. This is to allow the assessment of the association between the outcome variable and individual level characteristics. The model containing the individual level variables is used to determine whether the variation across communities could be explained by the characteristics of the individuals residing within that community or not.
Yij = β0j + β1 X1ij+...+βn Xnij+ u0j+eij............2
In the above model: β0j is the intercept, β1 is the regression coefficient (regression slope) for the explanatory variable, X1ij is number of individual’s level factors and eij is the usual (random error term).
A third model contains only the community level characteristics to allow the assessment of community level variables on the outcome variable.
Yij = βoj +β1Z1 + …+βnjZnj+eij + unj ……………………………………3
Each cluster has different intercept βoj, slope coefficients β1 , Znj is number of Community level factors, and unj random residual error terms at the cluster level.
Fourth model includes explanatory variables at both the individual and community level simultaneously. The simultaneous inclusion of both individual and Community level predictors in the multilevel logistic regression model permits: (1) the examination of Community effects after individual level confounders have been controlled for: (2) the examination of individual level characteristics as modifiers of the community effect and (3) the simultaneous examination of within and between Community variability in outcomes, and of the extent to which between community variation is explained by individual and community level characteristics.
The formula for the final model is expressed as:
Log [Pij / (1-Pij)] = βoj +β1X1ij + β1Z1j+…..+ uoj+ eij
Pij is the probability of LBW ith birth weight in the jth Area
β0j is the log odd of the intercept
β1, β... βnj are the regression coefficient estimate the data
X1ij,…Xnij are the covariates (independent variables) which may be defined at the individual level
Z1j,…Znj are the covariates (Area variables) which may be defined at the Area level
uoj are random error at the Area level
eij are random error at the individual level
Parameter estimation method
The parameters that have to be estimated are the fixed coefficients β0, β1, etc and the random parameters σ²u0.
In the multilevel model, fixed effects (measure of association) refer to the individual and community covariates and expressed as Adjusted Odds Ratio (AOR) and 95% confidence interval. The random effects are the measure of variation on LBW across communities. The ratio of the variance at the community level to the total variance is referred to as the intra-class correlation coefficient (ICC). The precision is measured by the standard error (SE) of the independent variables [19].The result of random effects (which are the measure of variation) are expressed as Variance Partition Coefficient (VPC) (which in this study is equal to ICC), and proportional change in variance (PCV). As a result of the dichotomous nature of the outcome variable in the study, the VPC is calculated based on the linear threshold model method which converts the individual level variance from the probability scale to the logistic scale [20]. In other words, by using the linear threshold model, the unobserved individual outcome variable follows a logistic distribution with individual level variance, i.e. σ²e = to π²/3 (=3.29). In this case, the VPC corresponds to the ICC, which is a measure of general clustering of individual outcome of interest in the communities.
The ICC is calculated as: ICC = (σ²u/(σ²u+ π²/3)
ICC is the proportion of community variance out of the total variance (Community plus individual variance) where σ²u is the variance at community level, π² /3=3.29 is the individual level variance.
Community differences with LBW may be attributable to contextual influences or differences in individual composition of communities (including unobserved individual characteristics). In view of this, while adjusting for the individual characteristics in the multilevel model, same part of the compositional differences were taken in to consideration to explain some of the community difference observed in the empty model. Thus the equation for the proportional change in community variance is:
PCV1= (VN1-VN2)/VN1
VN1 –is the Community variance in the empty model and VN2 is the community variance in the model including either individual level characteristics or Community level characteristics or both individual and Community level characteristics [20].
The Wald test was used to test the null hypothesis that a parameter value is zero or that a group of parameters are jointly zero. The latter case applies when testing the significance of categorical variable. Linear functions of parameters can also be tested. If the null hypothesis is true, the test statistic is distributed as approximately x² with r degrees of freedom, where r is the number of functions that are being tested [21]. Hence, the significance of freedom variation at each level will be tested with the Wald test, and p- values <0.05 were considered to be significant to reject the null hypothesis.
Model diagnostics
Multi-collinearity diagnostic evaluation was done using variance inflation factor (VIF), and thus value of VIF greater than 10 was considered as evidence of problematic multicollinearity. Interaction effects were assessed between individual and Community level explanatory variables [22].
Model fit statistic
Receiver operating characteristics (ROC) curve was used to assess general accuracy of the model to the data set using the area under receiver operating characteristics. ROC curve is a commonly used measure for summarizing the discriminatory ability of a binary prediction model. Relative goodness-of-fit tests were conducted using Akaike’s information criteria (AIC) for each of the models and compared. AIC is better in situations when a false negative finding would be considered more misleading than a false positive (for sensitive model). AIC is the appropriate information criteria to measure relative goodness of fit in multilevel modeling [23].
Results
In this study, all the descriptive part tables and proportions are weighted unless indicated as un-weighted; because the EDHS data was coming from strata and clusters that are sampled disproportionately and for this reason the DHS manual recommends weighting to make the sample more representative. In this study, missed values for continuous variables were managed by replacing the mean value of normally distributed variables and median value of not normally distributed variables. For missed categorical values, similarly, we substituted using mode value of the variable under consideration. The variable husband/partner educational level were found to have maximum missed values (6 missed values) and no other independent variable is found to have more than 2 missed values.
Individual level characteristics of the study participants
A total of 2110 children nested within 445 clusters were included in the analysis. Among which 13% of the children were with low birth weight. Children born to mothers single tone were 2045 (96.9%) and 65 (3.1%) were born from multiple birth. 2047 (97%) children were born at term gestational age and 63 (3%) mother’s gave birth at preterm phase. Most (80.07%) children born alive during the survey were from non-anemic mothers and the rest were born from anemic mothers.
Majority (38%) of the children was born from mothers with primary education, 698 (33%) from mothers with secondary/higher level education and the rest are from mothers who have not formal education (Table 1a).
Community level characteristics of the study participant
When we see the proportion of live births weighted and reported in different regions of Ethiopia, majority (28.5%) were found in Oromia followed by the SNNP region (21.2%). Afar region has the smallest (0.44%) number of live birth weighted and reported compared to the other regions in Ethiopia (Table 1b).
Multivariable multilevel logistic regression analysis
This multilevel modeling was used to determine the predictors of LBW and to assess how much of the variations observed between the communities were explained by the variables considered in the model.
The random effect (Table 2) revealed significant variability in the odds of low birth weight across the communities (clusters) σ²υ= 0.434, p< 0.001). In the model building, the empty model, that had no predictor variable, showed that the proportion of variation on the low birth weight explained by the clustering effect was 11.12% that enabled us to justify the use of multilevel modeling in this analysis.
The final model for LBW, that contained both the individual and Community level variables, were found to be the best model relative to the other models. The test statistics in table 2 indicated that the value of AIC, which is used to estimate the goodness of fit of consecutive models, were 1469.67, 1340.07, 1463.08 and 1333.33 for model 1, model 2, model 3 and model 4 respectively. From this, model 4 is with the lowest AIC value justifying the final model fit better to explain the data in this analysis. The area under ROC curve was 0.7297; indicating the model predicts well. Therefore; all the associations and discussions that would be done in this document was based on the findings from the final best model (model-4).
Controlling for both the other individual and Community level variables in model 4, children whose mothers with multiple birth were 2.74 times (AOR=2.74; 95%CI: 1.450- 5.184) more likely to be LBW compared to children born from mothers with single birth (Table 2).
The gestational age at birth was also maintained its significance level as well as its odds ratio after controlling the individual and community level predictor variables. Those children with preterm birth were 4.83 times (AOR= 4.83; 95%CI: 2.644-8.830) more likely to be LBW compared to children born with full term birth (Table 2).
Moreover, the odds of low birth weight amongst children born to anemic mothers were 1.49 times (AOR=1.49; 95%CI: 1.069-2.099) more likely to LBW compared to children born to non-anemic mothers (Table 2).
Birth order was also retained its significance after controlling both individual and the Community predictors in which the LBW were 58% (AOR= 0.42; 95%CI: 0.242-0.752) less likely to occur in children born with six and above birth order compared to children born at birth order of one up to three (Table 2).
Children born to mothers attained secondary and higher educational level were 61% (AOR= 0.39; 95% CI: 0.252- 0.612) and born to mothers attained primary educational level were 39% (AOR= 0.61; 95% CI: 0.418-0.896) less likely to have LBW compared to those children whose mothers had not attained any educational level (Table 2).
After adjusting both the individual and community level predictors, children born to mothers living in Afar, Amhara, Oromia and SNNP were 3.83 times (AOR = 3.83; 95% CI: 1.463-10.044), 3.50 times (AOR = 3.50; 95% CI: 1.649- 7.428), 2.19 times (AOR=2.19; 95% CI: 1.085-4.411), and 2.39 times (AOR= 2.39; 95% CI: 1.236-4.644) more likely to have LBW respectively compared to mothers living in Tigray region (Table 2).
Discussion
This study delivers important insights in to the low birth weight from Ethiopian demographic and health survey of 2016 data. The objective of this study was assessment of individual and community level factors associated with low birth weight. The discussion would be focusing on individual level and community level factors including statistical methods and strength and limitation of the study
NB: The discussion about multilevel factors is all about the findings from the final model (the best model selected using both AUC and AIC).
| Characteristics | Frequency weighted | % | Normal BW | LBW | LBW % |
|---|---|---|---|---|---|
| ReligionOrthodoxProtestantMuslimOthers | 100646962015 | 47.722.229.40.7 | 87142352215 | 13545980 | 1310160 |
| Age of mother (in year) 15-24years25-34 years35 and above years | 5361208366 | 25.457.217.4 | 4701037325 | 6617141 | 121411.2 |
| Member of at household1-56 and above | 1299811 | 61.638.4 | 1119712 | 18099 | 1412 |
| Sex of child MaleFemale | 10771033 | 51.148.9 | 960871 | 117161 | 1116 |
| Sex of HH head MaleFemale | 1681429 | 79.720.3 | 1476356 | 20573 | 1217 |
| Maternal age at 1st birthLess than 18 years18 and above years | 5571553 | 26.473.6 | 4791353 | 79200 | 1413 |
| Gestational age at birthTermPreterm | 204763 | 973 | 179734 | 25029 | 1246 |
| Child is single or twinSingle birthMultiple birth | 204565 | 96.93.1 | 179239 | 25226 | 1240 |
| Marital statusNot marriedMarried | 202090 | 199 | 171814 | 2276 | 1513 |
| Birth order1-34-56 and above | 1535318257 | 72.715.112.2 | 1342252237 | 1936620 | 13218 |
| Smokes cigarettesNoYes | 21028 | 99.60.4 | 18247 | 2771 | 1313 |
| Anemia level AnemicNot anemic | 3991603 | 19.980.1 | 3331397 | 66207 | 1713 |
| Mothers educational levelNo educationPrimarySecondary/higher | 609803698 | 28.93833.1 | 498714619 | 1118879 | 181111.3 |
| Maternal occupationNot Employed Employed | 1253857 | 59.440.6 | 1073758 | 17999 | 1411 |
| Husband education levelNo educationPrimarySecondary/higher | 414690878 | 20.934.844.3 | 339585791 | 7510789 | 181510 |
| Husband occupationNot Employed Employed | 9041078 | 45.654.4 | 747986 | 157110 | 1710 |
| Nutritional statusUnderweightNormalOverweight/obese | 2891361390 | 14.266.719.1 | 2331176355 | 5618535 | 19149 |
| wealth indexPoorMiddleRich | 3632941453 | 17.213.968.9 | 3062431283 | 5751170 | 161712 |
| Media exposure Not exposedExposed | 7131397 | 33.866.2 | 6111220 | 102177 | 1413 |
Table 1a: Low birth weight distribution by individual level characteristics, EDHS 2016, Ethiopia, 2020.
| Characteristics | Frequency weighted | % | Normal BW | LBW | % |
|---|---|---|---|---|---|
| RegionTigrayAfarAmharaOromiaSomaliBenshangulSNNPRGambellaHarariAddis AbabaDire Dawa | 29492886027336448121330629 | 13.960.4413.6428.533.441.7121.210.570.6314.491.36 | 27272245236533389111227126 | 2226479845911353 | 7222213111113881110 |
| ResidenceUrbanRural | 10261084 | 48.6351.37 | 914917 | 112167 | 1115 |
| Community povertyLowHigh | 1424666 | 67.4732.37 | 1244588 | 18097 | 1314 |
| Community education LowHigh | 2001109 | 94.835.17 | 173893 | 26316 | 1315 |
| Community media exposureLowHigh | 10521058 | 49.8850.12 | 895937 | 157121 | 1511 |
Table 1b: Low birth weight distribution by community level characteristics, EDHS 2016, Ethiopia, 2020.
| Characteristics | Empty Model 1 | Individual Model 2 AOR (95% CI) | Community Model 3 AOR (95% CI) | (Individual & Community) Model 4 AOR (95% CI) |
|---|---|---|---|---|
| Child is single or twin Single birth Multiple birth | Ref3.25(1.670-6.355) | Ref2.74*(1.450-5.184) | ||
| Child is single or twin Single birth Multiple birth | Ref3.25(1.670-6.355) | Ref2.74*(1.450-5.184) | ||
| Birth order1-34-56 and above | Ref0.80(0.501-1.296)0.40(0.205-0.801) | Ref0.87(0.570-1.326)0.42*(0.242-0.752) | ||
| Gestational age Term Preterm | Ref6.69(3.361-13.35) | Ref4.83*(2.644-8.830) | ||
| Anemia level Not anemic Anemic | Ref1.37(0.974-1.954) | Ref1.49*(1.069-2.092) | ||
| Mothers educational level No education PrimarySecondary/higher | Not anemic0.61(0.396-0.941)0.43(0.252-0.752) | Ref0.61*(0.418-0.896))0.39*(0.252-0.612) | ||
| RegionTigrayAfarAmharaOromiyaSomaliBenishangulSNNPRGambelaHarariAddis AbabaDire Dawa | Ref3.98*(1.509-10.499)3.74*(1.762-7.950)2.23*(1.113-4.483)1.93(0.957-3.891)1.13(0.54-6-2.371)1.92(0.999-3.707)1.79(0.890-3.602)0.74(0.340-1.629)1.96*(1.030-3.760)1.32(0.667-2.637) | Ref3.83*(1.463-10.044)3.50*(1.649-7.428)2.19*(1.085-4.411)1.32(0.625-2.818)1.35(0.630-2.906)2.39*(1.236-4.644)1.71(0.846-3.471)0.73(0.330-1.623)1.73(0.935-3.203)1.23(0.627-2.437) | ||
| Random effect parameters | Empty | Individual | Community | Individual and Community |
| Community level variance and (SE) | 0.434(0.1869) | 0.300(0.1801) | 0.247(0.1572) | 0.155(0.1576) |
| ICC (%) | 11.7 | 8.4 | 7 | 4.5 |
| PCV (%) | Ref | 33.6 | 44 | 64.3 |
| Model fit statistics AIC | 1469.67 | 1340.07 | 1463.08 | 1333.33 |
| The empty model contains no variables but partitions the variance into two component parts, SE= Standard error, ICC= Intra class correlation coefficient, PCV= Proportional change of in variance, AIC= Akaike's information criterion, Ref= Reference, AOR=Adjusted Odds Ratio and CI=Confidence interval. | ||||
Table 2: Multivariable multilevel logistic regression analysis of individual and community level factors associated with low birth weight, EDHS 2016, Ethiopia, 2020.
Figure 1
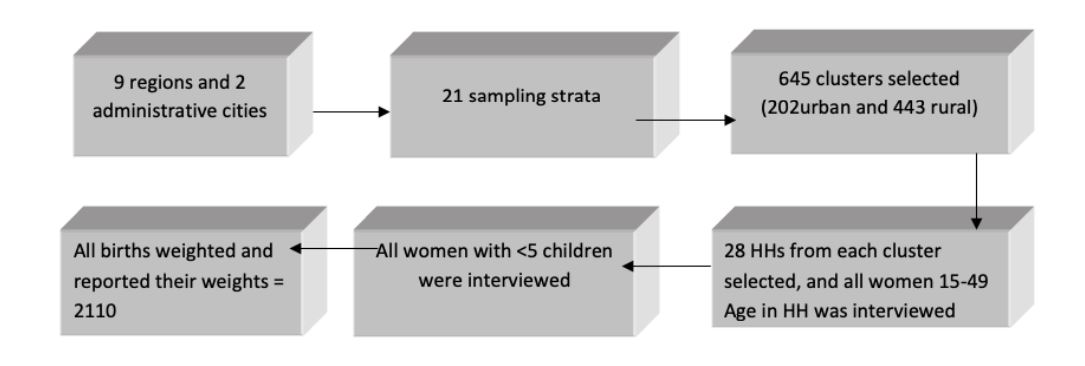
Figure 1: The individual level (lower level) variables are nested under the community level (higher level) variable where both level variables could have the potential to affect the outcome variable, low birth weight.
Individual level factors
At the individual level, factors such as the type of birth, gestational age at birth, anemia status, birth order and mother’s educational level were found to have a significant association with low birth weight.
Child whose mother’s with multiple births had high odds of LBW compared to those with single birth. Study done in Nigeria also shows multiple birth children were found to be significantly positively associated with LBW [24]. Similarly, a multilevel analysis conducted in Ethiopia also showed that multiple-birth children are 1.964 times more likely to have a LBW than single births [25]. Twin gestations are commonly associated with delivery of LBW infants because sometimes leading to complications like anemia, high blood pressure and early labor that could lead them to have low birth weight [26]. This high odds of low birth weight in multiple births could be due to sharing of all the nutritional and hormonal demands between those multiple neonates that was intended for single tone gestation.
Gestational age at birth was also found to be an important factor in determining low birth weight in this study. Preterm gestational ages at birth had higher odds of low birth weight compared with full term birth. Studies conducted in Tanzania, Ghana and Uganda also shows gestational age less than 37 weeks were found to be significantly positively associated with LBW [27-29]. This is also consistent with study conducted in Gondar, Ethiopia [30]. This could be due to shortage of time to develop the conception to the level of normal birth weight.
This study found that anemic mothers were positively associated with low birth weight. Similar studies conducted in northern Tanzania and Ethiopia also shows mothers who are anemic are significantly vulnerable to small birth size than those who had not anemic mothers [25,31]. Some studies have demonstrated a strong association between low hemoglobin before delivery and LBW babies. Maternal anemia is commonly considered a risk factor for LBW babies [32]. This low birth weight among anemic mothers may be due to lack of getting enough oxygen and other nutrients necessarily essential for the conception growth.
Even though having a birth order of 6 and above showed odds of low birth weight compared to lower birth order (one up to three), other study conducted in Malawi revealed that birth order of 2–3 and 4–5 are associated with lower risk of being small at birth compared to those with first birth order [33]. But another studies conducted in 2014 in Ethiopia revealed birth order of the child appeared to have no significant effect on determining the baby’s size at birth [25]. During pregnancy, structural changes take place in the uterine spiral arteries, increasing blood flow with beneficial effects for fetal growth [34]. This inconsistent finding may be due to differences in sample size and accuracy of data.
Maternal educational level appeared to be a very important determinant of the LBW in this study. The risk of LBW is significantly higher for children whose mothers have no education than children whose mothers have primary or secondary/higher level of education. Other studies done in Northern Tanzania, Nigeria, Kenya and Malawi implied that mothers’ education has an association with delivery of LBW. Children of higher education mothers have reduced chance of being small at birth than children of mothers with no education [24,27,33,35]. Previous single level studies done in Ethiopia showed a consistent result with this study [25,36]. Low educated mothers are more frequently malnourished, have unhealthy habits, chronic diseases and inadequate prenatal care and this in turn related with mothers delivering small birth size infants [25].
Community level factors
Of the community (cluster) level variables, only region was found to be significant predictor of low birth weight.
Concerning the regional disparity children born in Afar, Amhara, Oromiya and Southern nations, nationalities and people were at a higher odds of LBW than children who born in Tigray. Similarly, previous study conducted In Ethiopia showed that children whose mothers reside in Afar, Amhara and Addis Ababa were more likely to be LBW as compared to those from the reference category (Dire Dawa) [25]. The observed high odds of LBW in these regions may be attributed to differences in nutrition, socio-economic status, health care services, and other cultural and life style differences among these regions.
Statistical method discussion
ROC curve as measure of goodness of fit: Using predict probability, xb command in STATA, prediction is done based on only fixed effects. In this situation the AUC is a measure of goodness of fit which uses only fixed effect for prediction as AIC do. So, both are expected to give consistent decision. In this study, the final model was found to have relatively good fit, from both AIC and AUC values.
Strength and limitation
Strength: DHS data has individual (women) level sampling weight that is used to weight the descriptive part to make it more representative.
Limitation: DHS data has no cluster level weighting which is, in multilevel modeling, necessary for performing weighted analysis (for the analytical part).
Some variables included in the model might not be collected at the same date of the event occurrence
In addition to the common weakness of crosectional study design the above limitations are particularly important.
Conclusion
In this study the overall percentage of low birth weight in Ethiopia remained higher. The results of this study showed that multiple births, anemic mothers, birth order, not-educated mothers and preterm gestational age at birth were significant factors of low birth weight. Also, there exist considerable differences in baby’s size at birth among regions. Hence, switching off/on the significant factors accordingly could reduce the risk of having low birth weight child.
Declarations
Acknowledgment
We are grateful to thank Mekelle University, College of Health Science, and Department of Biostatistics, Tigray Regional Health Bureau and central statistical agency (CSA) for their support during this study.
Funding
Partially funded by Mekelle University
Ethics approval and consent to participate
Ethical approval was obtained from the research ethics review committee of Mekelle University, College of Health Sciences and the consent to participate was guaranteed by the ethics review committee and DHS program since an already existing data were used. However, confidentiality, and privacy of the data were assured.
Availability of data and materials
The dataset used in this study had not been released to public. According to relevant regulations, the data cannot be shared publicly. However, it can be obtained from the corresponding author up on reasonable request.
Authors’ contributions
Kibrom Taame Weldemariam, the principal investigator, has participated in designing and planning of the research; and in extraction and analysis of the data as well as in preparing the manuscript. Dr. Haftom Temesgen Abebe, Kebede Embaye Gezae and Tsegay Tekulu Tsegay have participated in planning, designing and analyzing the study. All authors read and approved the final manuscript.
Consent for publication
Not applicable
Competing interests
We all authors declared that we have no competing interests.

View pdf
Download pdf
View pdf
Download pdf
WHO (2011) Optimal feeding of low birth weight in infant low and middle income countries. Department of maternal, child and adolescent health. Geneva, Switzerland.[ Ref ]
Rajaeefard M, Mohammadi M Choobineh A (2007) Preterm delivery risk factors: a prevention strategy I Shiraz, Islamic Republic of Iran. Eastern Mediterranean Health Journal 13: 551-559.[ Ref ]
CSA (2016) Ethiopian Demographic and Health Survey. Addis Ababa, Ethiopia.[ Ref ]
Kliegman R, Behrman R, Jenson H, Stanton B (2008) Nelson textbook of Pediatrics. Elsevier, Philadelphia.[ Ref ]
UNICEF, WHO (2004) Low birth weight: Country regional and global estimates. New York.[ Ref ]
Sharma M, Mishira P (2013) Maternal risk factors and consequence of low birth weight in Infant. OSR Journal of Humanities and Social Science (IOSR-JHSS) India 13: 39-45.[ Ref ]
Deshpande D, Phalke B, Bangal B, Peeyuusha D, Sushen B (2011) Maternal Risk Factors for Low-Birth-Weight Neonates: A Hospital Based Case-Control Study in Rural Area of Western Maharashtra, India. National Journal of Community Medicine India 5: 394.[ Ref ]
The Government of Tigray National Health Bureau, The Government of Tigray National Health Bureau. (2013) Tigray regional health bureau annual profile, 2013: Mekelle.[ Ref ]
WHO (2014) Global Nutrition Targets 2025: low birth weight policy brief. WHO.[ Ref ]
Blencore H, Cousen S, Oestergaard M (2012) National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. The Lancet 379: 2162-2172.[ Ref ]
WHO (2012) Born too soon: the global action report on preterm birth. Geneva, Switzerland.[ Ref ]
Uthman OA (2007) Effect of low birth weight on infant mortality: Analysis Using Weibull Hazard Model. The Internet Journal of Epidemiology 6: 8.[ Ref ]
Marchant T, Willey B, Katz J, Clarke S, Kariuki S, et al. (2012) Neonatal Mortality Risk Associated with Preterm Birth in East Africa, Adjusted by Weight for Gestational Age: Individual Participant Level Meta- Analysis. PLoS Medicine 9: e1001292.[ Ref ]
Lawn JE, Osrin D, Adler A, Cousens S (2008) Four million neonatal deaths: counting and attribution of cause of death. Paediatr Perinat Epidemiol 22: 410-416.[ Ref ]
United Nation System (2007) The sixth report in the world nutrition situation. Geneva, Switzerland.[ Ref ]
Tema T (2006) Prevalence and determinant of LBW in Jima zone, Southwest Ethiopia. East African Medical Journal 83: 366-371.[ Ref ]
FDRE (2015) Health Sector Transformation Plan Ministry of Health.[ Ref ]
Stoltzfus JC (2011) Logistic Regression: A Brief Primer. Acadamic Emergency Medicine 18: 1099-1104.[ Ref ]
Antai D, Moradi T (2010) Urban Area Disadvantages and Under-5 Mortality in Nigeria: the effect of rapid urbanization. Environ Health Perspect 118: 877-883.[ Ref ]
Merlo J, Yang M, Chaix B, Lynch J, Rastam L (2007) A brief conceptual tutorial on multilevel analysis in social epidemiology: investigating contextual phenomena in different groups of people. Journal Epidemiology Community Health 59: 729-736.[ Ref ]
Goldstin H (2003) Multi statistical models. Arnold, London.[ Ref ]
Vatcheva KP, Lee M, McCormick JB, Rahbar MH (2016) Multicollinearity in Regression Analyses Conducted in Epidemiologic Studies. Epidemiology (Sunnyvale) 6: 227.[ Ref ]
Hox J (2010) Multilevel Analysis. Techniques and Applications. Utrecht University, The Netherlands.[ Ref ]
Dahlui M, Azahar N, Oche OM, Aziz NA (2016) Risk factors for low birth weight in Nigeria: evidence from the 2013 Nigeria Demographic and Health Survey. Glob Health Action 9: 1-8.[ Ref ]
Betew W, Kebede E (2014) Determinants of Low Birth Weight among Children Aged 0 to 59 Months in Ethiopia. Int J Pure Appl Sci Technol 25: 14-25.[ Ref ]
Onyiriuka AN (2010) Low birthweight infants in twin gestation. Curr Pediatr Res 15: 01-06.[ Ref ]
Siza JE (2008) Risk factors associated with low birth weight of neonates among pregnant women attending a referral hospital in northern Tanzania. Tanzania Journal of Health Research 10: 1-8.[ Ref ]
Ishmael AB (2011) Assessing The Risk Factors Associated With Low Birth Weight (LBW) And Mean Actual Birth Weight Of Neonates: A Case Study Of St. Martin‟S Hospital, Agroyesum. Kumasi: Kwame Nkrumah University, Ghana.[ Ref ]
Louis B, Steven B, Margret N, Ronald N, Emmanuel L, et al. (2016) Prevalence and Factors Associated with Low Birth Weight among Teenage Mothers in New Mulago Hospital: A Cross Sectional Study. Journal of Health Science 4: 192-199.[ Ref ]
Zenebe K, Awoke T, Birhan N (2014) Low Birth Weight & Associated Factors Among Newborns in Gondar Town, North West Ethiopia: Institutional Based Cross- Sectional Study. Indo Global Journal of Pharmaceutical Sciences 4: 74-80.[ Ref ]
Mitao M, Philemon R, Obure J, Mmbaga TB, Msuya S, et al. (2016) Risk factors and adverse perinatal outcome associated with low birth weight in Northern Tanzania: a registry-based retrospective cohort study. Asian Pacific Journal of Reproduction 5: 75-79.[ Ref ]
Muhammad OA, Kalsoom U, Sughra U, Hadi U, Imran M (2011) Effect of Maternal Anemia on Birth Weight. J Ayub Med Coll Abbottabad 23: 2-3.[ Ref ]
Ngwira A, Stanley C (2015) Determinants of Low Birth Weight in Malawi: Bayesian Geo Additive Modelling. pLoSONE 1: 1-14.[ Ref ]
Khong T, Erwich J, Adema E (2003) On an anatomical basis for the increase in birth weight in second and subsequent born children. Placenta 24: 348-353.[ Ref ]
Omedi G, Amwoliza V (2014) Factors Associated with Low Birth Weights in Kenya. Journal of Research in Humanities and Social Sciences 5: 97-106.[ Ref ]
Gebremedhin S, Enquselassie F, Umeta M (2012) Independent and Joint Effects of Prenatal Zinc and Vitamin A Deficiencies on Birthweight in Rural Sidama, Southern Ethiopia: Prospective Cohort Study. PLoS ONE. 7: e50213.[ Ref ]
